Colby Joncas, BS and Raymond F. Sekula, Jr., MD
There has been a great deal of discussion recently about the “best” way to perform a microvascular decompression (MVD) for treating trigeminal neuralgia. Specifically, should Teflon™, glue, or neither be the preferred mode of treatment?
In this article we will explore the pros and cons of each technique and provide the information needed to help the reader understand why different procedures may be performed.
The History of Microvascular Decompression (MVD)
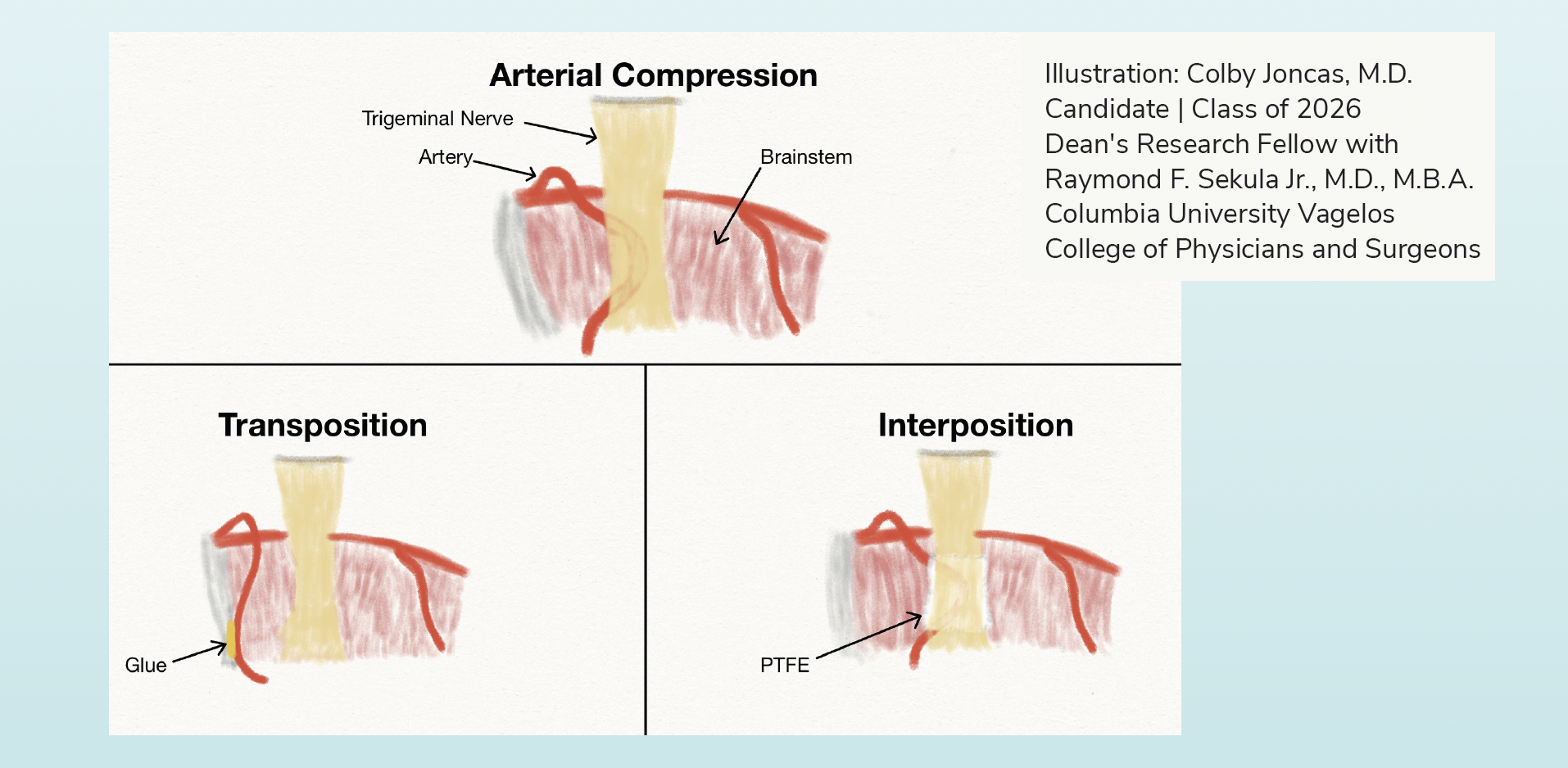
While a detailed description of the history of microvascular decompression is beyond the scope of this article, it is of interest that “Teflon-free” microvascular decompressions were performed as early as the 1960s. The first “Teflon-free” vascular decompression of the trigeminal nerve was performed by Dr. William Gardner, who separated an artery away from the trigeminal nerve with a piece of Gelfoam®, an absorbable and sterile sponge made from pigs. That was an example of an interposition surgical technique – a method wherein the surgeon inserts or interposes a piece of material between the nerve and the offending blood vessel. A few years later, Dr. Peter Jannetta described his own technique for microvascular decompression of the trigeminal nerve and incorporated the operative microscope. The “micro” portion of microvascular decompression denotes the use of the microscope to perform the operation. Dr. Jannetta described his technique as follows, “The artery could be freed from the fine to dense arachnoidal membranes, thus allowing the vessel to assume a new position away from the nerve.”(1). Thus, Peter Jannetta had described a “Teflon-free” transposition technique to treat trigeminal neuralgia – a technique wherein the surgeon relocates or transposes the offending blood vessel to alleviate contact between the nerve and vessel. In subsequent years, however, Jannetta and other surgeons noted recurrences of trigeminal pain in their patients and wondered if the cause was recurrent vascular compression because there was no permanent barrier between the nerve and offending artery.
In an effort to avoid this problem, surgeons began to interpose various materials, such as small pieces of muscle, fat, or plastic, between the trigeminal nerve and offending artery. In time, Dr. Jannetta began to use a kind of plastic, Teflon™, which was discovered in 1938 by the scientist, Roy Plunkett, PhD, working in the Dupont Labs. The chemical structure of Teflon™ is polytetrafluoroethylene (PTFE), and nowadays, it is manufactured and sold by many chemical and pharmaceutical companies. Over the years, various techniques for microvascular decompression using interposition and transposition techniques have been described, often with great enthusiasm.
In the past few decades, some surgeons have warned that interposition with PTFE or other implant material causes a kind of “neocompression” (i.e., meaning that the compression from the blood vessel is replaced by compression by the implant) of the trigeminal nerve. And more recently, some have argued that the use of Teflon™ can result in granulomas, which result in recurrences of pain. It is probably important to know that very few surgeons actually use TeflonTM made by Dupont’s subsidiary holding company, Chemours. Most surgeons use whichever PTFE is available through their hospital’s vendor agreements. Calling all PTFE products “Teflon” is like stating all forms of tissue paper are Kleenex™, which is only made by the company Kimberly-Clark. Is this an important distinction to make? We don’t know the answer to this question, but most scientists would agree that PTFE produced by different manufacturers likely results in different local immune responses which may or may not have any bearing on long-term outcomes.
Like interposition techniques, various transposition techniques for the treatment of trigeminal neuralgia have been described over the past few decades. Transpositions can be accomplished using various techniques that make use of materials such as dural slings, metal clips, or glue-like substances. And to make matters more confusing, many surgeons use PTFE or TeflonTM to perform transpositions by looping the material around the offending artery before securing it to another structure in the head.
What evidence exists in medical literature?
Several noteworthy studies have examined the relative efficacy of transposition versus interposition in microvascular decompression for trigeminal neuralgia. There remains considerable debate in the field as to whether interposition or transposition provide superior outcomes following microvascular decompression. In 2008 (this debate has been ongoing for decades!), Dr. Marc Sindou and colleagues published a study in Operative Neurosurgery examining 330 patients who underwent microvascular decompression for trigeminal neuralgia specifically examining pain outcomes as a result of operative technique (transposition versus interposition) (2). Of 260 patients undergoing transposition using a Teflon™ sling, 214 (82%) were pain-free, while 47 of 70 patients (67%) undergoing interposition were pain-free at a mean follow up of 8.2 years.
The authors, therefore, argued for the superiority of transposition over interposition. There are several problems with this claim. First, the authors state that transposition was essentially not possible in one-third of the patients (3). Second, the patients undergoing transposition had compression of the trigeminal nerve by the superior cerebellar artery (SCA). Many other studies have demonstrated that patients with compression of the trigeminal nerve by the SCA do better than other patients. These factors introduce significant bias into the study that limits the generalizability of its findings and likely lead to the misleading conclusion that transposition is categorically better than interposition.
In a much more balanced study published in the Journal of Neurosurgery in 2024, Uhl et al. compared 102 patients undergoing transposition and 100 patients undergoing interposition for trigeminal neuralgia (4). After a median 31.5 months followup, 85 patients (83.3%) in the transposition group experienced positive outcomes. After a median 95 months follow-up, 85 patients (85%) in the interposition group experienced positive outcomes. The reader should understand that there will be ongoing recurrences of pain in some percentage of patients undergoing both transposition and interposition. This rigorously conducted study found no difference in pain outcomes between the interposition and transposition techniques for microvascular decompression.
At this time, as seen in this study and considering the broader array of published articles examining this topic, there is no concrete evidence to suggest that one technique is better than the other.

Why do some surgeons believe a “Teflon-free” transposition is better?
Recently, some surgeons have argued that the formation of Teflon™ or PTFE granulomas in contact with the trigeminal nerve may be the cause of pain recurrence. Like any foreign body surgical implant, PTFE results in an inflammatory response to varying degrees. This is known as the foreign-body reaction. This is the body’s attempt to protect itself from foreign material of any kind. An example of a foreign-body reaction may help explain the process. When I was a child, I was running through a neighbor’s yard after dusk and lacerated my shin on a recently cut branch of a neighbor’s hedge. For months, the wound was painful, purulent, and unwilling to heal. After some time, my mother took me to the emergency department in my small town, and a doctor pressed deeply into my wound (it hurt!) and surmised that a foreign body must have been retained in the muscle over my shin during the accident. He painstakingly removed a small piece of fractured wooden branch from deep within the wound, and the wound healed within a week or so. For those few months after the accident, my body was attempting, but unable to expel an unsterilized foreign body.
In contrast, many modern surgical treatments (e.g., hip implants, heart valves, etc.) rely upon the integration of sterilized foreign implants in the body. In some cases, however, the body’s response to a sterilized foreign implant can be inappropriate. There are reports of perfectly performed hip implants associated with chronic and worsening inflammation resulting in bone loss and implant loosening ultimately requiring a revision surgery. And Teflon™ or PTFE implants have been used for nearly five decades in MVD surgery with little problem. But over the past two decades (i.e., a brief search of the worldwide literature returns nearly 50 publications concerning Teflon™ or PTFE granulomas), some neurosurgeons have argued that Teflon™ or PTFE granulomas are the cause of trigeminal neuralgia recurrences following MVD. So what is a “granuloma?” Granulomas are small, localized groupings of immune cells that surround or wall off an infection, injury, or foreign body. In MVDs performed with Teflon™ or PTFE, true granulomas occur in a very small number of patients. In these patients, the theory is that the Teflon™ or PTFE granuloma results in compression of the trigeminal nerve and may be responsible for the recurrence of pain. The argument is an attractive one and certainly easy to convey to patients. Certainly, Teflon™ or PTFE granulomas may be the cause of pain recurrence in a very small number of patients, but that number is exceedingly small. If it was a large number, the patients undergoing transposition without a Teflon™ implant against the trigeminal nerve in the Uhl et al. study described above should have fared better than those patients who underwent interposition with Teflon™ wrapped around the nerve, but they did not do better.
Why does pain recur in some patients after microvascular decompression? And will removal of Teflon™ or PTFE felt cure the pain?
The vast majority of MVD failures occur because preoperative workup was suboptimal. While there are many types of facial or trigeminal pain syndromes, MVD works best for those patients with short bursts of electrical pain and MRI evidence of neurovascular compression. Too often, we meet individuals in our clinics or through the FPA, who have undergone an MVD that likely should never have been performed. We can preoperatively predict with some certainty those patients for whom MVD will durably relieve pain (5). We recently learned of a patient who underwent an interpositional MVD and immediately awoke with pain. The patient requested transfer to a center in another state performing transpositional MVD. This is a problem of misinformation.
In those individuals, however, who have experienced a successful MVD for years and experience a recurrence, PTFE felt or TeflonTM granuloma may be the cause of recurrent pain in a small minority. And it should be noted that most neurosurgeons agree that the act of removing the PTFE or TeflonTM felt from a trigeminal nerve is, to varying degrees, injurious to the nerve, and the injury itself is the likely explanation for relief of pain as we know that various injuries using chemicals (e.g. glycerol), heat (e.g. radiofrequency), or radiation (e.g. GammaKnife or CyberKnife) result in, at least, temporary relief of pain in the distribution of the trigeminal nerve.
What is the best surgical option for me?
Many patients have questions about which technique is better: interposition or transposition. There is no simple answer to this question at this time. There are a variety of factors that may influence the decision to perform one technique or another, but often it is a decision that is made during surgery once the surgeon is able to see and assess the individual’s unique anatomy.
In our practice, we stopped using PTFE felt or Teflon™ in our patients approximately two years ago. When we do perform an interpositional MVD (less than 10% of patients), we avoid PTFE. We generally perform transposition with resorbable glue in a majority of cases for two reasons that both relate to management after microvascular decompression (6).
First, the detection of recurrent neurovascular compression of the trigeminal nerve after MVD by MRI is improved without the use of PTFE. Second, if for any reason surgery is required for re-exploration of the trigeminal nerve, we expect to find less scarring about the trigeminal nerve when PTFE or Teflon™ has been avoided in the first operation. This latter point, however, has never been rigorously studied.

References:
1. Jannetta PJ. Arterial compression of the trigeminal nerve at the pons in patients with trigeminal neuralgia. J Neurosurg. 1967;26(1):159-162. doi:10.3171/jns.1967.26.1part2.0159
2. Sindou M, Leston JM, Decullier E, Chapuis F. Microvascular decompression for trigeminal neuralgia: the importance of a noncompressive technique–Kaplan- Meier analysis in a consecutive series of 330 patients. Neurosurgery. 2008;63(4 Suppl 2):341-351. doi:10.1227/01.NEU.0000327022.79171.D6
3. Sindou M, Leston J, Decullier E, Chapuis F. Microvascular decompression for primary trigeminal neuralgia: long-term effectiveness and prognostic factors in a series of 362 consecutive patients with clear-cut neurovascular conflicts who underwent pure decompression. J Neurosurg. 2007;107(6):1144-1153. doi:10.3171/JNS-07/12/1144
4. Uhl C, Faraj L, Fekonja L, Vajkoczy P. Transposition versus interposition method in microvascular decompression for trigeminal neuralgia: midterm analysis of both techniques in a single-center study. J Neurosurg. 2024;140(6):1777-1784. Published 2024 Jan doi:10.3171/2023.11.JNS231658
5. Panczykowski DM, Jani RH, Hughes MA, Sekula RF. Development and Evaluation of a Preoperative Trigeminal Neuralgia Scoring System to Predict Long-Term Outcome Following Microvascular Decompression. Neurosurgery. 2020;87(1):71-doi:10.1093/neuros/nyz376
6. Joncas CT, McKhann GM, Sekula RF. Letter to the Editor. Concerning transposition for microvascular decompression in trigeminal neuralgia. J Neurosurg. 2024;141(5):1451-1452. Published 2024 Aug 23. doi:10.3171/2024.5.JNS241160